Our last day of the course, and the morning prayers were tinged with sadness. It’s been a fantastic two weeks, and I’ve made lots of genuine friends. I’m really going to miss going back to real life…
Dermatology
 Claire Fuller gave us our final topic session of the week, based on many years of experience in both the UK and East Africa.
Claire Fuller gave us our final topic session of the week, based on many years of experience in both the UK and East Africa.
The WHO is working with the Gates Foundation to run a Global Burden of Disease statistics measuring. 600 million cases of scabies worldwide. In the developing world, skin disease is the second commonest reason for attending primary care – but people are still far less likely to attend if they have a rash compared to other types of pathology.
As in many other areas, traditional healers cause many problems – their treatment for lymphoedema is to puncture the legs multiple times to let the fluid out. Sadly, this leaves the door wide open for infection.
Dermatological Examination
Important features to have.
- Suitable location for skin examination
- Satisfactory light
- Examine patient all over – check mouth, nails, scalp, feet, genitalia.
- Distribution of lesions.
The problem is, because don’t want to strip off because the clinic is full of people and no privacy, but then you take them down to the cupboard, and its too dark to see.
Bacterial skin disease
Very commonly this will be impetigo – yellow crust to blisters, generally around nose and mouth.
- They need to wash the skin – with clean waters and disinfectants. Remove crusts, debris and necrotic tissues.
- Apply antimicrobial preparation – herbal, honey, hydrogen perocide, chlorhexidine, topical antibiotic.
- Oral antibiotics – flucloxacillin, erythromycin.
Eczema
Eczema is very common in the developing world. Can be especially aggressive in African skin. Rather than simply affecting the flexures, it can affect the whole trunk, and can cause very high levels of inflammation, which leaves hypopigmentation after resolution.
Often needs emollients and dermovate.
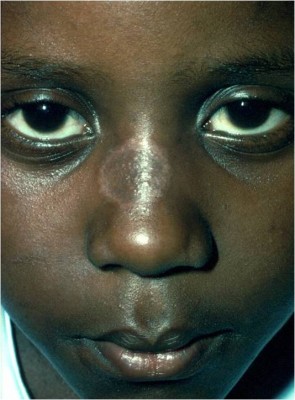
Tinea
Scaly round rashes on arms or trunk related to ring worm. Can be treated with topical antifungals. However, tinea capitis – affecting the scalp – will need systemic antifungals. (See image above on right)
Pyoderma, scabies and renal damage
There is an established association between scabies and pyoderma. In those with scabies + pyoderma, 5-10% will have visible haematuria: so it should be treated.
80% of dermatology consists of 8-10 common diseases. If it smells like pyoderma, it probably is.
Medical implications of skin-lightening products
These can cause local damage, with inflammation and awful stretch marks. In Malawi, around 5-10% of people attending our clinic had problems related to these creams.
Patients will deny using the products, so you have to say “I’ve heard that people who use these creams get these problems”, letting them save face.
HIV/AIDS
Having a skin disease is a risk factor for having HIV, from evidence in Tanzania. Multiple dermatoses is quite specific for low CD4 count. In one study, 88% of adolescents with HIV had a skin disease.
The best way to treat the HIV associated dermatopathology such as Kaposi’s Sarcoma is to treat the HIV.
Ulcers
- Treat underlying cause.
- Keep clean without dirsupting healing (antiseptic soaks, water fit for drinking is fit for wound case)
- Treat secondary infection
- Greasy covering prevents adhesion and good for pain relief.
- Compression is very helpful.
Removing suspicious lesions
[iframe width=”600″ height=”450″ src=”http://www.youtube.com/embed/7CzDEok8Wmo”]
Podoconiosis
 Known as “Podo” – one of the forms of elephantisis. Seen in the highlands of tropical countries with lots of bare feet in muddy professions.
Known as “Podo” – one of the forms of elephantisis. Seen in the highlands of tropical countries with lots of bare feet in muddy professions.
Skin swells and becomes woody and hard. Smells insanely awful. Basically an end stage lymphoedema.
Usually can be dramatically improved with frequent washing and antiseptic. Get children to wear shoes, prevents the condition occuring.
Our scheme in Ethiopia has led to all who are treated being invited to join the team to teach others. 30,000 have now been treated in the scheme!
Teaching… a workshop
Our closing session was from Vicky Lavy, talking us through the wonderful art of teaching, a key tool for all of us, especially in the developing world.
Many of us have done a fair amount of teaching. As a group we came up with lots of words beginning with E, about the important things that teaching needs to achieve:
 Enable
Enable- Enthuse
- Educate
- Empower
- Entertain
- Encourage
- Exchange
- Effect (on patient care)
- Everlasting (sustainability)
What makes a good teacher?
- Clear + interesting
- Acting
- Inventive
- Honesty
- Inventive
- Relevance
- Love for the subject
- Audience
- Approachable
- Knowledge + Preparation
- Experiment
Teaching tools
There are millions of different teaching styles: Participation, Lectures, Scenarios, Practicals, Groups, Role play, Mentoring, Informal, Teach others, Drama & Song, Quiz, Stories, Bed side, Shared consultations, Video, Books, Online, Visual stuff, Thought exercise, Buzz groups.
One week after a lecture, evidence shows that people often only remember around 20% of the information.
Some of these are very effective in developing settings, others not so well. Generally, developing world cultures are used to very didactic of teaching, which means they can learn by rote, but are not well versed in problem solving.
However, once they get used to small groups, which can take some time, they find them useful also. Good to tell people they can use their own language in the groups.
“I was doing some teaching in china, and trying to ask questions, and just getting blank faces. However, over the 3 days, the group slowly opened up, talking about patient cases. By the end, I found they were very engaged.”
- Dealing with wrong answers – Important to a) not embarrass people, but also b) correct dangerous treatment ideas.
- Breaking up teaching sessions is valuable – to keep people awake. Having a buzz group session between talks is helpful. A buzz group is where someone turns to their neighbour and briefly discusses an issue
- Visual aids – showing pictures, to tell stories. One teacher on this course has showed us the manacles used to hold psychiatric patients to the wall. That kept us awake!
Case example: Teaching student nurses in Uganda about immunisation within 1 hour
We broke into lots of pairs and tried to come up with teaching sessions. Then fed back to the group. Huge variation in styles and approaches. Some groups taught basic practical skills, some came up with dramas, some had very ambitious plans to teach a much more holistic community engagement approach.
Closing
Ian’s closing remarks: God did not make us to cope with burdens on our own. Jesus sent people out two by two, not individually. We need to share our burdens together.
We then all held hands and closed in prayer together.
And that’s all folks. Sad to feel we are at an end, but I’ve definitely never enjoyed a medical course, or generally teaching so much. I’d like to give some huge thanks to Vicky and Ian, and the whole of the CMF team. Bless you all!