Whilst I drove to Oak Hill College, I listened to Radio 4, with a very relevant Thought for the Day, that I’ve completely forgotten. If I get an opportunity, I will look it up. I then drank lots of apple juice, then sat in the lecture hall…
The Global Picture of HIV
 Gisela Schneider opened the day on HIV. She told us two stories, one of a bishop at a national conference, washing the feet of those with HIV, and another, of a pastor apologising, in tears, to a woman who said how she has been unable to speak publically about her HIV status. The pastor apologised, because Christians too easily judge it as a moral problem, and forget that there are people in the midst of it who simply need the love of Christ.
Gisela Schneider opened the day on HIV. She told us two stories, one of a bishop at a national conference, washing the feet of those with HIV, and another, of a pastor apologising, in tears, to a woman who said how she has been unable to speak publically about her HIV status. The pastor apologised, because Christians too easily judge it as a moral problem, and forget that there are people in the midst of it who simply need the love of Christ.
When she first worked in Gambia in the 80s, HIV arrived, but it was simply referred to as “the disease”. No-one would talk about it, no one would accept it, and it was simply hoped that the patients would die and take away the shame from the family. The Lancet article in 1985 was the first to describe a hetrosexual disease spread by sexual contact. At that time, patients simply died.
We have seen a wonderful precedent in the speed that civil society identified that ARVs needed to be patent free. If left to pharmacutical industry, ARVs would not be patent free until 2016 – whereas since 2000 we have actually had more than 6 million people started on treatment.
We asked our clinic users what they wished to be called by us. They did not want to be “patients”, or “clients”. They said “Call us friends”. We must be in a partnership to defeat HIV.
In global politics, HIV is beginning to be seen as a resolved problem: governments are starting to reduce funding, public interest is waning: new causes such as global warming are taking a place on the global agenda. We must fight to keep a public interest alive in HIV. If not, funding will be cut, patients will not recieve medications, and a treatment resistant form of the disease will spread, unopposed.
There have been some successes – 20% reduction in HIV Transmission from 2006-2011. The numbers of infected people are stablising, but there are still 7,000 new infections a day worldwide.
Some examples, of the varying leading risks for infection.
- Lesotho – stable heterosexual couples
- Kenya – multiple partners
- Benin – sex workers
In Lesotho, being married is the best indicator of risk for HIV infection!
Africa is ahead of the game. In places such as India and the rest of Asia, there are some shocking statistics – in Lahore, 82% of sex workers did not think they were at risk of HIV infection.
History of HIV
- 1981: First AIDS case reports
- 1984: First HIV tests
- 1990: First HAARTs
- During 80s & early 90s: the focus was on Prevention. Scaring patients, increasing awareness. This wasn’t terribly effective. Spending on AIDS globally was around 200 million.
- Late 90s & 00s: we began aiming for Universal Access, with a political backing. The key change was DOHA, which created a mechanism to allow WTO members to issue compulsory licences to export generic versions of patented medicines to countries with poor. Spending on AIDS globally is now around 20 billion.
One downside is that drug companies are now showing hesitancy to invest in HIV treatments due to the risk they will have their drugs stolen as generic drugs, and make no money.
Discussion: What are the main challenges in HIV today?
- Western economic crisis, increasing instablity in Africa leads to programmes falling apart.
- Primary Care settings, often the drugs are not available.
- Some places, such as PNG, are way behind the curve.
- Sustaining the enthusiasm politically and locally.
- Treatment has meant that people are less scared of the disease, and more complacent.
- Stigma is still a huge problem.
- Cultural norms, gender inequalities.
Stigma is worldwide. In Germany in 2012, a lady from Togo with HIV and Cervical cancer, wasn’t being treated for the cancer, because the Gynacologists were scared to operate due to the virus.
The New Approach – SAVE
Safe practices – ABC, Circumcision, Safe infections, etc.
Access to treatment – Reduction in Viral load reduces transmission, PMTCT, etc.
Voluntary counselling and testing – Stigma free counselling, etc.
Empowerment of children, women and youth – families, communities, leadership, PLWHA, etc.
“The greatest good you can do for another is not just to share your riches, but to reveal to them their own.”
Benjamin Disraeli
HIV Basics
A tea break, before she sent all the experts out, leaving just the idiots like me who don’t know anything about HIV…
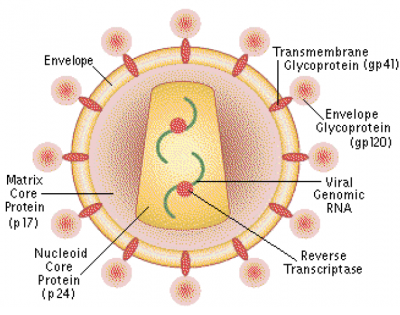
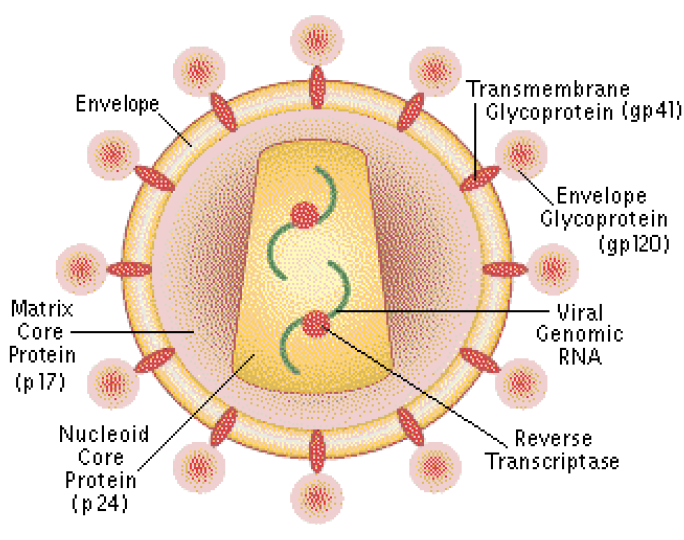 There are a number of different viruses involved, HIV1 M, HIV N, HIV O, HIV 2. The process of CD4 infection is through CD4 attachment, then Co-receptor binding with gp120 joining to surface proteins, with gp41 joining to CCR5 receptors in the cell wall, allowing the RNA inside to be released into the cell.
There are a number of different viruses involved, HIV1 M, HIV N, HIV O, HIV 2. The process of CD4 infection is through CD4 attachment, then Co-receptor binding with gp120 joining to surface proteins, with gp41 joining to CCR5 receptors in the cell wall, allowing the RNA inside to be released into the cell.
Once inside the cell, the RNA is integrated into the DNA of the cell, creating provirus. This process takes several days. This is the point at which lifelong infection begins. Once the RNA is integrated into one cell, the virus (currently) cannot be eradicated from the body.
The initial stage, of introduction of RNA to the cell takes around 2 hours – some preventative drugs work on this process – which is why post exposure prophylaxis ideally needs to happen within 2 hours.
 Once CD4 cells are infected, they become disorganised. They are still there, but they can no longer react to immune problems correctly. Over the next 12 weeks, the virus is replicated, sometimes causing an acute viral “conversion” syndrome – click the graph on the right for a larger version. There is an excellent explanation of this process that Gisela mentions in her slides at The Naked Scientist.
Once CD4 cells are infected, they become disorganised. They are still there, but they can no longer react to immune problems correctly. Over the next 12 weeks, the virus is replicated, sometimes causing an acute viral “conversion” syndrome – click the graph on the right for a larger version. There is an excellent explanation of this process that Gisela mentions in her slides at The Naked Scientist.
Testing is a key area of discussion, with the basics of 5Cs – Consent, Confidentiality, Counselling, Correct testing, Linked to Care.
Telling a patient they have HIV is so life changing, so painful, that you should not test patients if you cannot provide them with this fivefold support.
After infection, progression to an AIDS syndrome can take <5 years (10-20%), 7 years (60-70%), >10-15 years (5-10%). Less than 1% do not progress.
WHO staging
She advised us to print this list, and laminate it. We won’t be able to remember it, but we can refer to it as we see patients.
Stage I
Asymptomatic
Stage II
- Moderate weight loss (<10%)
- Recurrent respiratory infections (sinusitis, bronchitis, otitis media etc)
- Herpes Zoster
- Angular cheilitis, oral ulcers and sores
- Papular pruritic eruptions (PPE)
- Seborrhoeic dermatitis
- Fungal infections of nails
Stage III
- Unexplained weight loss >10%
- Unexplained chronic diarrhoea > 1 month
- Unexplained persistent fever > 1 month
- Persistent oral candidiasis
- Oral hairy leukoplakia
- Pulmonary tuberculosis
- Severe bacterial infections (e.g. pneumonia, empyema, meningitis, pyomyositis etc)
- Acute necrotizing ulcerative stomatitis, gingivitis or periodontitis
- Unexplained anaemia (<8g/dl), neutropaenia (<0.5 x 109/l), thrombocytopaenia (<50 x 109/l)
Stage IV
- HIV wasting syndrome
- Pneumocystis pneumonia (PCP)
- Recurrent severe bacterial pneumonia
- Chronic herpes simplex infection (> 1 month)
- Oesophageal candidiasis
- Extrapulmonary tuberculosis
- Kaposi’s sarcoma
- Cytomegalovirus infection (retinitis or other organ)
- Central nervous system toxoplasmosis
- HIV encephalopathy
- Extrapulmonary cryptococcosis
- Disseminated non-tuberculous mycobacterial infection
Case studies of HIV
Gisela then walked us through some case studies, through common presentations of ?HIV patients. Opportunistic infections – important markers for clinical stages. Need to be treated before initiating ART:
Fever of unknown origin – commonly due to TB, Malaria, PCP, Cyptococcus, Toxoplasmosis.
Focal neurological lesions – commonly due to Toxoplasmosis, Tuberculoma, Primary CNS lymphoma, Brain abscess, Stroke.
Diarrhoea – less common now in areas with high ARV treatment, but in ARV naive areas, commonly due to Cryptosporidium, Microspora, Cyclospora, Isospora.
Basic preventative therapy:
Good studies showing that provision of the following can make a difference – but the community needs to be involved, as had been said all week. Go to a village, given them nets, they won’t use them. Work with a village, if they ask for help, then it becomes part of the village culture.
- CtX prophylaxis.
- Malaria protection (ITN).
- Clean water supply.
- Condoms.
- Nutritional support.
Anti Retrovirals Therapy
 A 5 minute break during which people laughed on hearing that the BMA just passed a motion calling for Andrew Lansley to resign. Then back to ART…
A 5 minute break during which people laughed on hearing that the BMA just passed a motion calling for Andrew Lansley to resign. Then back to ART…
Nucleoside Reverse Transcriptase inhibitors (NRTI)
- Backbone of therapy.
- Side effects of Anaemia (AZT), Polyneuropathy(D-drugs), lipatrophy, lactic acidosis.
Non Nucleoside Reverse Transciptase inhibitors (NNRTI)
- NVP – Can cause hypersensitivity, lead in. Hepatotoxic
- Efavirenz – Teratogenic.
Protease Inhibitors
- 2nd line treatment (but first for HIV 2). More expensive but effective.
- Difficult to take due to side effects – Diarrhoea bad. Also cause hypergylcaemia and hyperlipidaemia, long term cardiac risk.
Combination Therapy
- Generally two types, combined. Commonly 2 NRTI + 1 NNRTI. Sometimes 2 NTRI + PI.
- Important to avoid some combinations due to side effects.
Response to ART
Threefold improvements:
- Virological – Ideally level falling to an undetectable viral load.
- Immunological – Rise in CD4 count, around 10/month.
- Clinical – Weight gain, Disappearance of symptoms.
Highest risk of ART toxicity will be in the first 1-3 weeks. After this, the next few months 16% of patients in stage 4 starting ART will respond with an IRIS (Immune Reconstitution reaction). Common cause is CMV, TB or cryptococcal disease. Highest risk of death in in the first 3 months, worsened risk by low CD4 count – can be avoided if we start treatment early!
Treatment Failure
Clinical treatment failure: a new or recurrent stage IV event.
Immunological treatment failure: fall of CD4 to baseline. 50% fall from peak. Persistent low levels of CD4.
Virological treatment failure: viral load > 5000 copies.
ART Counselling
Counselling is one of the most important factors in useful ART treatment. You need cultural sensitivity, there must be understanding, real communication and community support. Indigenous health workers are the most effective at this, so they can be the best contributors to good compliance.
HIV in Pregnancy and Childhood
Lots of Quorn sausages later, I walked through the gardens barefoot in the 27 degree heat, chatting about Somalia with a fellow CMFer, and wishing that there was ice-creams. Then we returned to the expert world of Gisela…
“No child should be born with HIV, no child should be orphaned from HIV, no child should die from HIV”
11 year old HIV orphan, Ebube Taylor, speaking to a UN panel
48% of eligible adults are receiving ARTs. Only 23% of eligible children receive ART.
Seven year follow up of Gambian pregnant women living with HIV-1. Mothers who died within 7 years: 34%. HIV infected children who died 69%. Orphans who died irrespective of their HIV status. In other words: being an orphan is as bad for your mortality as being a child with HIV.
Reducing vertical transmission

20% of maternal deaths in Africa are due to HIV. Avoid this by using ART, and aiming for quick normal deliveries, avoiding instrumental delivery. Where feasible, elective CS.
Ideally start combined ART for all pregnant women, continuing for life. Some places use a single dose nevirapine to prevent mother-to-child transmission – but there is a widespread resistance to this. When mother on ART, breast is best, and relatively safe!
Mother on ART throughout pregnancy reduces transmission from 30-40% to 2%.
Childhood HIV
- Category 1: Die within 1 year. (25%-30%)
- Category 2: Symptoms early in life, die aged 3-5 (60%)
- Category 3: Develop symptoms >age 8. (10-15%)
Test all children with a dried blood spot test with the first review after birth. HIV children present commonly in first year of life with PCP. Treat with high dose ABx.
Treating children is very complex. Much better to heed Ebube Taylor’s words, and prevent vertical transmission.
Palliative Care in Resource Poor Settings
 Unsurprisingly, the 27 degree heat, coupled with 5 hours of very intense discussion of medications with long names and scary side effects, I nearly fell asleep. 2 pints of coffee later, and AC turned on in the lecture theatre, I steeled myself for our final lecture from CMF’s own Vicky Lavy.
Unsurprisingly, the 27 degree heat, coupled with 5 hours of very intense discussion of medications with long names and scary side effects, I nearly fell asleep. 2 pints of coffee later, and AC turned on in the lecture theatre, I steeled myself for our final lecture from CMF’s own Vicky Lavy.
Vicky spent several years establishing and running Paediatric Palliative Care in Malawi. She then wrote a Palliative Care toolkit for use by others, and much of her teaching is from that.
A nurse we had been working with for several months said “Doctor, I do not see how this Palliative Care can work – the patients, they just keep dying!”
Caring rather than curing. A revolutionary concept to many places in the world.
Palliative care is looking after people with illnesses that cannot be cured, relieving their suffering, and helping them through difficult times. The “care” is key. As Jesus said:
“When I was sick, you looked after me”.
Matthew 25:36.
In the developing world, very often Doctors say “There is nothing we can do”. But Palliative Care never says this – no matter how small, there is always something we can do.
Counselling and psycological support is a vital part of palliative care. Often forgotten in favour of exciting discussions of oxycodone doses, but actually is probably more important. Truth is one of the most powerful medicines available to us, but we still need to develop a proper understanding of the right timing and dosage for each patient. Despite cultural differences, there are studies across the world showing that telling patients the truth has a positive medical effect.
Pain management should be done by the mouth, by the clock, by the ladder. Oral, regularly, and according to the WHO pain ladder. Codeine is very expensive, so we usually pass from Step 1 to Step 3 quite quickly.
Top tips
- Topical metronidazole for smelly wounds. Smelly wounds are stigmatising, but just crush metronidazole can resolve problems.
- Metronidazole pessary for vaginal discharge. Similar to above, with Cervical Ca
- Opiates for breathlessness and diarrhoea.
- Gentian Violet paint for candida and skin sores.
- Prednisolone for mouth ulcers.
- Franjipane juice for Herpes Zoster. Common African flower, sticky juice inside a flower.
Taking a spiritual history
Always something that can be helpful, but a very important part of Palliative Care
- “I ask everyone about this, as part of our routine assessment.”
- Do you have a faith which helps you through difficult times?
- Do you ever pray?
- What helps you make sense of life?
- What things are most important to you?
- Have your thoughts about life changed since you became ill?